Write to the elected representatives that represent you. These are the elected officials that are on the ballot for your district. Don’t waste time writing to elected representatives in other states or in other places. Politicians care about their own constituents — people who are eligible to potentially vote for them, and who they are elected to represent. Representatives disregard contact attempts from people who are not in their district. Writing to government agencies, outside their prescribed application or public comment processes, is also not typically helpful. Writing anonymous letters or posting anonymous comments on social media are also generally not effective. Representatives care about what their actual verifiable constituents care about.
This constant reelection pressure means that MoCs are enormously sensitive to their image in the district or state, and they will work very hard to avoid signs of public dissent or disapproval.
There is a dangerous new government policy being proposed which could harm healthcare workers and patients across the country. Instead of strengthening infection control policies in healthcare settings to protect workers and patients from infectious diseases, the CDC is planning future guidance which could lower healthcare infection control standards.
HICPAC meets up to 8 times a year at CDC in Atlanta, Georgia. Meetings are open to the public and time for public comments is allotted on the agenda. See the Meeting Information page for planed meeting dates and registration information.
Maintaining masking requirements for HCP during all direct clinical encounters may marginally reduce the risk for transmission from HCP to patient or from patient to HCP. Those potential incremental benefits, however, need to be weighed against increasingly recognized costs. Masking impedes communication, a barrier that is distributed unequally across patient populations, such as those for whom English is not their preferred language and those who are hard-of-hearing and rely on lip reading and other nonverbal cues.
This woke-washing tactic is being used to promote anti-mask arguments and gin up opposition to N95 use in healthcare settings. Erica Shenoy might just be vain and maybe wants people to see her face, but she claimed in an Annals of Internal Medicine op-ed that dropping masking for infection control in healthcare is needed so that patients would be able to lip read - the innuendo being that masking is somehow discriminatory toward the hard of hearing. This is astonishingly foolish woke-washing since lip reading only has a 30% to 40% accuracy rate. Even trained professional lip readers only attain perhaps 60% accuracy. Doctors should surely never depend on lip reading for receiving critical medical advice with such a large potential for miscommunication.
Lip-reading on its own isn’t enough. It is estimated that only 30% to 40% of speech sounds can be lip-read even under the best conditions and extra information is usually required to understand what is being said. So while it can be an important skill for children with a hearing loss to have, relying on lip-reading alone will not be enough for your child to develop good communication skills.
Lip-reading is a notoriously tricky business with professionals only able to decipher what someone is saying up to 60% of the time. "Machine lip-readers have enormous potential, with applications in improved hearing aids, silent dictation in public spaces, covert conversations, speech recognition in noisy environments, biometric identification and silent-movie processing," wrote the researchers.
I’m not feeling isolated, Erica. I don’t pine longingly to see my doctor’s lips because I’m not a weirdo. I have my own family and so does my doctor. I have neighbors and friends and hobbies, and a life to live. And I’d like to continue with all that by avoiding viruses disrupting my life on top of whatever else I need to see the doctor about. My doctor and I don’t need to stare at each other’s unmasked faces in the exam room. I go there for healthcare. And most of us certainly don’t want to get covid if already in a state to need the hospital. It’s obviously bad to add covid on top of another condition — you’d think a doctor would know about comorbidities, or has heard of the often repeated “underlying conditions” reference, or as the CDC describes it, People with Certain Medical Conditions who are at higher risk of covid complications.
If you’re travelling to a malaria-endemic area, a mosquito net should be on your list of essential travel supplies. Malaria is transmitted by the female Anopheles mosquito that bites humans from dusk to dawn. The Anopheles mosquito is stealthy and silent. They don’t buzz so you can’t hear them approaching. This means you are a prime target when you are most vulnerable — asleep. Bed nets are a key defence against malaria, but they also offer protection from other diseases such as filariasis (known for massive swelling of the limbs) and other insects and arachnids like ticks, beetles, flies, and spiders. Remember that in malarious areas, insecticide-treated mosquito nets are required in bedrooms without tightly-fitting window screens or broken screens Bed nets are not required in buildings with sealed windows and central air conditioning.
Signing a covid waiver for legal liability is required for attending “packed to the brim” APHA event. “Packed to the brim” seems like a peculiar choice of words for what they know is going to be rife with the spread of infectious disease. And we know that they know the virus will spread there, not because they are public health experts, but because they spell it out in the legal covid waiver that attendees must agree to, as shown by @danaludwig. It stipulates attendees “risk exposure to and contraction of potentially dangerous diseases and viruses” and that “APHA makes no representations that it has taken any safety precautions that relate to infectious diseases or exposure.”
Many insurers have implemented changes in response to the pandemic. These have included price increases, new exclusions and other risk reduction measures. Further, insurers classified the COVID pandemic as a “known event” in January 2020. This classification is assigned after an unexpected or unforeseen event occurs, and it removes future coverage in many instances.
I went to a doctor's office today (wearing N95 like about half of the other patients) and none of the medical staff were wearing any masks at all. The staff required each patient to sign this waiver acknowledging how dangerous Covid-19 is, and how they might infect us!
HCP [Health Care Personnel] entering the AIIR [Airborne infection isolation room] soon after a patient vacates the room should use respiratory protection. (See personal protective equipment section below) Standard practice for pathogens spread by the airborne route (e.g., measles, tuberculosis) is to restrict unprotected individuals, including HCP, from entering a vacated room until sufficient time has elapsed for enough air changes to remove potentially infectious particles (more information on clearance rates under differing ventilation conditions is available). We do not yet know how long 2019-nCoV remains infectious in the air. In the interim, it is reasonable to apply a similar time period before entering the room without respiratory protection as used for pathogens spread by the airborne route (e.g., measles, tuberculosis). In addition, the room should undergo appropriate cleaning and surface disinfection before it is returned to routine use.
Use respiratory protection (i.e., a respirator) that is at least as protective as a fit-tested NIOSH-certified disposable N95 filtering facepiece respirator before entry into the patient room or care area. See appendix for respirator definition.
(6) CDC has issued the document, Interim Infection Prevention and Control Recommendations for Patients with Known or Patients Under Investigation for 2019 Novel Coronavirus (2019‐ nCoV) in a Healthcare Setting (Attachment A), in an effort to prevent the spread of infection during healthcare delivery. This guidance is not intended for non‐healthcare settings (e.g., schools) OR to persons outside of healthcare settings.
(7) This guidance is based on the currently limited information available about 2019‐nCoV related to disease severity, transmission efficiency, and shedding duration. This cautious approach will be refined and updated as more information becomes available and as response needs change in the United States.
(8) The CDC has also provided two checklists: Hospital Preparedness Checklist (Attachment B) and Healthcare Providers Preparedness Checklist (Attachment C). These are available to aid healthcare facilities in preparing to receive and evaluate potential cases or persons under investigation (PUIs)s for 2019‐nCoV.
That is focused on two things. One, we do not know the extent of contribution that environmental virus might pose. And so the glove and gown use is with an eye towards ensuring that we don't accidentally transmit infection that way. Eye protection is something that we, I think, culturally for a generation or more, have been lax about. I think that's, frankly unacceptable in routine times, given that influenza spreads wildly across our community every year. And so this, as well as for routine practices, is an opportunity to firm up our use of eye protection. It's not about there being necessarily target epitopes in the conjunctiva. It's the fact that our eyes drain into the back of our throats and if you're trying to keep respiratory viruses out of your throat, then protecting your eyes makes sense. Nose and mouth, similarly, need to be protected. We use respirators in this context because of the very likely possibility of a contribution of near range inhalation. This is something we've talked about with every concerning respiratory infection over the past 20 years. And that is the idea that when we cough or breathe, we generate a range of particle sizes. Some of them are big and splashy and can land directly on us. But if you're not within line of sight or ballistic range - but within about six feet - it's conceivable that somebody can be generating small particles with infectious material in them, that could drift in and be breathed and entrained in what you're inhaling. For that reason, a surgical mask that's a nice barrier against ballistic impact, isn't as good of a device. The fact that there's a half-inch gap on either side of your face really doesn't protect against inhalation. And so that's why we recommend respiratory protection. There is - there's always discussion of the available published evidence and ongoing generation remedies, that question what is the relative benefit of a mask versus a respirator. And I think the jury is still out. It seems to be fairly close, when we've compared respiratory infections across the board. But then again, there's always a question of adherence. And what we see is that people are much more likely to adhere correctly to surgical mask use than to respirator use. So that behavioral component is a bit of a question mark. We also are hearing early information about public issues that are upcoming that might show a lean towards maybe a little bit more protection with a respirator. So, I think we as a profession will continue to have to navigate that grey zone. But for the time being, that is the recommendation that we made during the containment phase.
Engineering controls involve isolating employees from work related hazards. In workplaces where they are appropriate, these types of controls reduce exposure to hazards without relying on worker behavior and can be the most cost-effective solution to implement. Engineering controls for SARS-CoV-2 include:
Installing high-efficiency air filters.
Increasing ventilation rates in the work environment.
Installing physical barriers, such as clear plastic sneeze guards.
Installing a drive-through window for customer service.
Specialized negative pressure ventilation in some settings, such as for aerosol generating procedures (e.g., airborne infection isolation rooms in healthcare settings and specialized autopsy suites in mortuary settings).
Administrative Controls
Administrative controls require action by the worker or employer. Typically, administrative controls are changes in work policy or procedures to reduce or minimize exposure to a hazard. Examples of administrative controls for SARS-CoV-2 include:
Encouraging sick workers to stay at home.
Minimizing contact among workers, clients, and customers by replacing face-to-face meetings with virtual communications and implementing telework if feasible.
Establishing alternating days or extra shifts that reduce the total number of employees in a facility at a given time, allowing them to maintain distance from one another while maintaining a full onsite work week.
Opponents have said the changes, detailed in a presentation in June, are based on a flawed evidence review and omit key infection control tools. Some have called attention to a CDC approval process that they say is sometimes inscrutable to the public.
Nathanael Nerode: “Loeb 2022 has been debunked multiple times and I have emailed the debunkings to you. And in addition Loeb failed to disclose a conflict of interest. Loeb was personally responsible for preventing Canadian nurses from getting access to KN95 masks which may well have injured and killed them. He did not disclose this conflict of interest; this makes all of his work suspect. In addition many of these studies listed there, including Loeb 2022 contained protocols that assumed the droplet dynamic which is now discredited and known to be false.”
“OSHA has a statutory responsibility, statutory requirement to have an open and transparent process like we are having today to just determine what the standard should be. CDC is a black box. We have no idea how these recommendations are determined. Unfortunately, until there are, there are Freedom of Information Act requests or Congressional inquiries. So given all those things, it's really incumbent upon OSHA to develop standards, and to say these are the standards that every employer covered by the standard must follow.”
Internal government emails obtained by The Associated Press show there were deliberate decisions to withhold vital information about new mask manufacturers and availability. Exclusive trade data and interviews with manufacturers, hospital procurement officials and frontline medical workers reveal a communication breakdown — not an actual shortage — that is depriving doctors, nurses, paramedics and other people risking exposure to COVID-19 of first-rate protection. Before the pandemic, medical providers followed manufacturer and government guidelines that called for N95s to be discarded after each use, largely to protect doctors and nurses from catching infectious diseases themselves. As N95s ran short, the Centers for Disease Control and Prevention modified those guidelines to allow for extended use and reuse only if supplies are “depleted,” a term left undefined. Hospitals have responded in a variety of ways, the AP has found. Some are back to pre-COVID-19, one-use-per-patient N95 protocols, but most are doling out one mask a day or fewer to each employee. Many hospital procurement officers say they are relying on CDC guidelines for depleted supplies, even if their own stockpiles are robust.
But the decline of in-person shopping and work, combined with factory shutdowns in places like China, disrupted the economy. A 2020 report from the corporate consulting firm McKinsey & Co. found the hardest-hit industries would take years to recover. One sector in particular that took a big hit was the fossil fuel industry. Oil demand fell sharply in 2020, placing the global economy on uncertain footing. Before long, business-aligned groups — particularly those connected to fossil fuels — began targeting the public health measures threatening their bottom lines. Chief among them were groups tied to billionaire Charles Koch, owner of Koch Industries, the largest privately held fossil fuel company in the world. The war on public health measures began on March 20, 2020, when Americans For Prosperity (AFP), the right-wing nonprofit founded by Charles and David Koch, issued a press release calling on states to remain open.
tweet by @jackmurphylive says “If covid had been left to do it’s thing our nation would have become as a result, healthier, fitter, and younger - ie stronger. 10:32 PM 11 December 2021
I came across a particularly aggressive anti-mask account on twitter in early 2021. He made a ridiculous capitalist fever dream argument to justify duping people into unmasking and getting sick, and maybe dying, for business interests. It seemed so blatantly ridiculous. Tweet from @reubenR80027912 dated 1019 am May 7, 2021 says Main Street is Very simple. Do 3 things PSA campaigns that you won’t die if vaxxed. Remind people kids aren’t a risk. Remove masks everywhere so people don’t constantly live in fear. Voila. Roaring economy. Spending is about freedom from fear. Quote-tweet from same account on February 22, 2021 says There’s something to the Mad Men pilot and covid. Telling people they’re more likely to die in a car accident than covid doesn’t matter. Nor do vax stats. Happiness is freedom from fear, a billboard that screams whatever you’re doing is ok @ DKThomp
The upside down call is coming from inside the house. And if the CDC pretty much just sanctions punitive measures against students to prevent masking in school, and disseminates anti-science nonsense immunity comments, how can we trust they won’t start pushing that we all need to breathe dirty air too? I don’t know what’s going on at the CDC, but I’m starting to wonder if there’s an awful lot of people who burrowed in from the Trump administration, because they all sound the same as the people in 2020 who said the elders should sacrifice themselves on the altar of The Economy - that people should just get back to work as the virus spread.
Knowing that COVID-19 has not gone away, some people are not yet prepared to let their guard down, according to a working paper distributed by the National Bureau of Economic Research. Some 13% of U.S. workers said they will continue social distancing as the economy opens up and cases fall, and another 45% said they will do so in limited ways. Only 42% said they plan a “complete return” to the activities they participated in before the pandemic.
COVID-19 Vaccination and Mask Requirements. Health care workers were praised for their self-sacrifice in caring for sick patients at the beginning of the COVID-19 pandemic, but then they were fired if they objected to receiving COVID- 19 vaccines with or without complying with onerous masking requirements and regardless of whether they already had the virus and had gained natural immunity. With the disease being endemic and constantly mutating, vaccines and universal masking in health care facilities do not have appreciable benefits in reducing COVID-19 transmission throughout the community. Moreover, more recent COVID strains pose fewer health risks than the earlier strains, and the pandemic has been declared to be at an end. CMS should:
- Announce nonenforcement of the Biden Administration’s COVID-19 vaccination mandate on Medicaid and Medicare hospitals.
- Revoke corresponding guidance and regulations.
- Refrain from imposing general COVID-19 mask mandates on health care facilities or personnel.
-Pay damages to all medical professionals who were dismissed directly because of the CMS vaccine mandate.
COMMENT ON MEDPAGE TODAY: With guidelines like that it just sounds as though CDC is attempting to ensure its own future existence (due to all the distrust and the post-pandemic public outcries for its dismantle/demise or at the very least a complete overhaul) by creating conditions absolutely ripe for starting as many potential epidemics as it possibly can, starting from within the hospital setting where it can spread easily into the community, thus going into the business of population reduction/control instead of infection control.
My name is Chloe Humbert. I don't want to be forced into exposure to multiple infections when I need to seek healthcare. I almost died from infection twice in my life because of inadequate investment in healthcare in 2 different countries. If we are to be forced into preventable exposure to covid and other diseases in healthcare settings, against our will, the goal of this forced infection needs to be spelled out, along with clearly stating the known consequences so the American people can say whether we want to bear those consequences. You can’t just rip away the freedom of individuals to protect ourselves from disease, and not have a clearly articulated reason, because the masks off, let it rip plan sounds an awful lot like the “natural herd immunity” garbage we heard in 2020 and the American people said no to that already. There are other names for this ideology and it’s a pseudoscience that patriots like my father, my uncle, and my step-father, all fought in a war to protect us from 80 years ago. Do not make guidelines that give cover for genocidal negligence in our hospitals and nursing homes. People in healthcare settings need to wash their hands and put on a mask and have air quality engineering controls to prevent disease spread in healthcare. Universal masking and broad use of N95 respirators in healthcare and essential spaces is a simple and valuable investment to save lives and that’s what I think we should do as a civilization.
Transcript:
I'm Chloe Humbert and I'm not waiting for everybody. And you don't have to either.
It's not worth pestering civil servants or government agencies to try to change the rules because they can't. uh somebody down at your local welfare office somebody at the health department they're there to provide uh stuff but they're not capable of changing the rules because somebody calls up and says hey that doesn't make sense or hey that's not fair that's not how it works uh they take orders from above and they have to abide by the laws and the policies set forth by your lawmakers, by the governors, by the president, by Congress, by your state legislators. So going to a public employee is not going to yield results and people get frustrated with this. So there are a couple exceptions to this and it's very specific. When there's an application that you can, if you, there's a form you can fill out that can do something. If you're reporting a spotted lanternfly in Pennsylvania, there's a public form where you upload the picture of it, you tell where the spotted lanternfly is. But otherwise, just sending, like, angry anonymous emails to the CDC or the FDA is just not going anywhere. That's just not... And tweeting at these agencies is even less effective. Or whatever it's called now. Sorry, Twitter.com, X, Twitter, whatever. When you do that, there's no... You're not attached to anything. When you write to your elected representatives, You're putting your address on there. They know you're a constituent. Your congressperson knows that you're in their district. And they're very sensitive to that. But some civil servant working, just doing a job, they just aren't going to be able to do anything about what you're upset about. They can't change the rules. Those come from, again, laws, policies that are decided by elected representatives or within the agencies, there are committees, but that is where we come to the public comment process. So this is not all the time, but when an agency is doing something to make changes or make a new guideline, They put out information about it and then they have a process that you can submit comments. Sometimes there's a public meeting and you can register to give oral comments. Sometimes it just calls attention to the issues and puts pressure on these agencies to know that people are involved and engaged. And it can make a difference. I would recommend also writing your elected representatives about any of the issues that you make comments on so that to let them know where you stand and what you think needs to happen at these agencies because there are committees, for example, in the Senate or Congress who oversee these agencies. The CDC recently had their HICPAC meeting. HICPAC stands for Healthcare Infection Control Practices Advisory Committee. Now this is the committee who makes the guidelines that the CDC puts out for healthcare infection control practices. So that would be things like stopping the spread of MRSA or COVID or any of those things that spread in health care and the ways to stop them. So we're talking masks, gloves, hand washing, disinfection. Strangely, the recent HICPAC meeting barely touched upon COVID, which is amazing because people are getting COVID in the hospital and it apparently has you know much more devastating effects because of course by the very reason that you're in the hospital means that you have other conditions so this is a problem first of all second they did accept public oral comments but they limited the time so there were a lot of people who signed up to give public comments and didn't get a chance to comment, including myself. I was at the meeting ready to give my public comment and I was not chosen. I'm going to play the public comment of Liv Grace and I think more people need to hear this.
Liv Grace is now your turn for public comment. My name is Liv Grace. I'm 36 and physically disabled as well as chronically ill. I have a number of autoimmune diseases, including lupus, and I already live with many of the conditions associated with long COVID such as POTS, lung disease, and kidney disease. Additionally, I'm immunodeficient on top of the immunosuppression for my lupus medication. I'm also a cancer survivor. People often comment that I live with so much illness and they say how hard that must be, but what is many times more difficult is being unable to safely access medical care. Last December, I caught RSV from my infusion center because my nurse, who knew she had been exposed to RSV, refused to wear an N95. That turned into pneumonia. Two weeks after recovering and returning to my infusions, I caught COVID there, just a few days before my birthday in February, after two months of recovery time from pneumonia. I then caught COVID a second time, while getting necessary post-COVID blood work in April, barely after covering from February's infection. One way N95 masking is not enough for me. I have not gotten medical care since April because of the reality that I will get sick again as long as medical providers refuse to practice respiratory hygiene. I attempted many times to implement ADA accommodations that would allow me to wait in my car rather than the waiting rooms and would require medical staff to wear an N95 while treating me. Over and over again, medical establishments refused. My appeals were rejected. I was told that it was impossible to accommodate my needs as a high-risk, severely immunocompromised person. I am still recovering from back-to-back COVID. I now suffer from increased kidney issues and new heart issues. I had to start taking a blood thinner and a statin to reduce my risk for a catastrophic cardiovascular event. Without medical care, my health will deteriorate to the point of needing hospitalization, where I will have even more exposure to unmasked staff. This is a catch-22. Either access care and catch COVID and other dangerous to me infections to the point of further endangering my life, or do not get care at all and endanger my life. The evidence review on N95 respirator and surgical mask effectiveness was flawed and must be redone with input from scientific researchers and experts in respiratory protection, aerosol science, and occupational health. This is eugenics. I'm Jewish and I see the writing on the wall, the history of not only the Holocaust, but many genocides, including the ongoing genocide of indigenous people target disabled people first. I am literally begging for something to be done. Thank you.
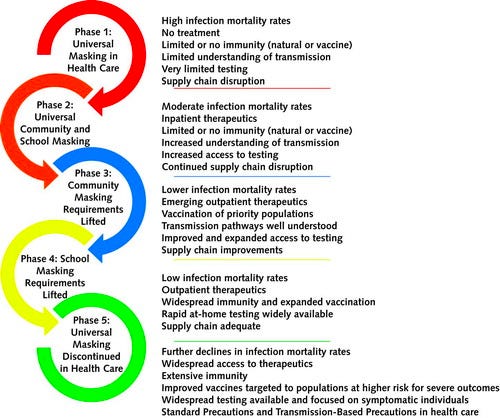
What are we doing? We have patients who need to give public comment at a CDC meeting, pleading with the CDC to advise their doctors not to give their patients COVID. What are we doing? Patients should not have to beg the CDC to advise doctors and hospitals not to force COVID on their patients. Erica Shenoy is on the HICPAC committee and this is a person who claimed in an op-ed in the Annals of Internal Medicine that dropping masks for infection control and health care is needed so that patients would be able to lip read. The innuendo being that masking is somehow discriminatory toward the hard of hearing. This isn't astonishingly foolish woke-washing because lip reading only has a 30-40% accuracy rate. Even trained professional lip readers only attain maybe 60% accuracy according to what I've been reading. Doctors should never depend on lip reading for critical medical advice. There's a 40 to 70 percent chance of failure to accurately communicate. That's not good odds. And this argument in the op-ed seriously suggests facial expressions for non-English speakers too. So this just sounds like it's all to let the hospitals off the hook for both for providing masks to health care workers, and also to get out of providing interpreters apparently. Just it doesn't make sense. And Shenoy's article also has this weird graphic that is supposed to demonstrate somehow the process of making COVID endemic where infection control is just abandoned because the supply chain situation is semi functional. So like if the supply chain economics is not completely broken down, then there's no reason for infection control anymore I guess is the takeaway here. They frame it as a process to endemic phase and phasing out all infection control which doesn’t make any sense. And it’s shocking that somebody who’s supposedly knowledgeable about infectious disease would even suggest this and that they wouldn't understand that when a disease is endemic, it means permanent infection controls. Where malaria is endemic, they don't stop using mosquito nets. Mosquito nets are mandated in hotels there. Where mosquitos carry disease you want to keep doing things to mitigate that? This should be obvious. I don't know where this goes to where you abandon. No. There’s whole organizations that fund mosquito nets for regions with endemic malaria. So endemic does not mean that you just say oh forget it now the supply chain is ok so who cares about human lives right. No. Does not make sense. And I saw online on social media somebody had posted a COVID waiver. Now I've seen these posted, you know, about concerts or conventions where you basically, you know, sign it and you agree to get COVID there because they know it's going to spread. So they want to take away your legal claims to any damages. This person posted a you agree to get COVID waiver. at the doctor's office. He said, and I quote, I went to the doctor's office today wearing an N95 like about half of the other patients and none of the medical staff were wearing any masks at all. The staff required each patient to sign this waiver acknowledging how dangerous COVID-19 is and how they might infect us. This person posted a picture of the text from the COVID waiver he signed and it said, By signing this agreement, I acknowledge the contagious nature of COVID-19 and voluntarily assume the risk that I may be exposed to or infected by COVID-19 by visiting the clinic and that such exposure or infection may result in personal injury, illness, permanent disability and death. I understand that the risk of becoming exposed to or infected by COVID-19 at the clinic may result from the actions, omissions, or negligence of myself and others including, but not limited to, staff, employees, the physician, representatives, or other patients visiting the clinic. I voluntarily agree to assume all the foregoing risk and accept sole responsibility for any injury to myself, including but not limited to personal injury, disability, and death, illness, damage, loss, claim, liability, or expense of any kind that I may experience or incur in connection with my visit to the clinic. On my behalf, I hereby release covenant not to sue, discharge, and hold harmless the clinic, its staff, employees, physicians, representatives, patient, or anyone visiting the clinic of and from the claims, including all liabilities, claims, actions, damages, costs, or expenses of any kind arising out of or relating thereto. I understand and agree that this release includes any claims based on the actions, omissions, or negligence of the clinic, its employees, physicians, representatives, patients, or anyone visiting the clinic, whether a COVID-19 infection occurs before, during, or after my clinic visit. So this is what health care providers want you to agree to. They want to forcibly give you COVID and then not have any responsibility for the consequences. I don't know what healthcare is for anymore other than to make money I guess because this flies in the face of any reason you would have a healthcare system. If you don’t care about making people sick, why would you even bother having a healthcare system. If you don’t. Why would you become a doctor if you like want to make people sick? Why would you have a healthcare system if the point isn’t to stop sickness? I don't know. But this is where we are. And clearly regulation is needed to stop these people from infecting everybody on purpose. It's really disheartening to think that we're told we're supposed to be OK with, you know, just getting sick a lot, even if it's not serious, because, you know, just being sick at all is not great. And you shouldn't be getting sick by going to the doctor. That shouldn't be a thing. One concept I see mentioned and bandied about is this idea that CDC doesn't know about airborne transmission of COVID, or that the CDC is stuck in droplet dogma. And that is, seems to be the case. But because if they're saying surgical masks are appropriate for COVID wards, that's, that's just not okay, if that's what they're planning on doing, which apparently floated at a former HICPAC meeting. So Nicholas Smit is in the elastomeric mask industry and he was lobbying for them to acknowledge elastomerics for quite some time and I found his research shows that the CDC knew back in 2020 that there was aerosol transmission happening. And they didn't get it wrong. They they knew this because they issued this information in January of 2020. In January 2020, the CDC put out guidance for the 2019 novel coronavirus. And this was January of 2020. And the New Jersey Department of Health also referred to this guidance at the time. And in it, It says, quote, healthcare personnel entering the airborne infection isolation room soon after a patient vacates the room should use respiratory protection. Standard practice for pathogens spread by the airborne route is to restrict unprotected individuals, including healthcare personnel, from entering a vacated room until sufficient time has elapsed for the air exchanges to remove potentially infectious particles. We do not yet know how long 2019-n-cov remains infectious in the air. In the interim, it is reasonable to apply a similar time period before entering the room without respiratory protection as used for pathogens spread by the airborne route, example measles tuberculosis. In addition, the room should undergo appropriate cleaning. This can't be clearer. They also say in this publication, use respiratory protection that is at least as protective as a fit-tested NIOSH certified disposable N95 filtering facepiece respirator before entry into the patient room or care area. So that six foot droplet stuff came about later. That was something that was added on. They knew. They knew about airborne precautions and also the precautionary principle. And in March 2020 at a HICPAC meeting, this is a quote from that. A surgical mask that's a nice barrier against ballistic impact isn't as good of a device. The fact that there's a half inch gap on either side of your face really doesn't protect against inhalation. And so that's why we recommend respiratory protection. So that's the quote. In March 2020, OSHA also put out guidance on preparing workplaces for COVID-19 and they included engineering controls, installation of high efficiency air filters, increasing ventilation rates in the work environment, installing physical barriers such as sneeze guards, installing a drive-thru window for customer service, encouraging sick workers to stay home, An article in MedPage Today says CDC advisory group under fire for proposed infection control guidelines. Nurse union, occupational health experts, patients, say weaker guidelines help only the employers. By Sophia Putka, August 24th, 2023. This says, quote, opponents have said the changes detailed in a presentation in June are based on a flawed evidence review and omit key infection control tools. Some have called attention to a CDC approval process that they say is sometimes inscrutable to the public. And this is true. Or as Dr. David Michaels, former OSHA head said, the CDC is like a black box. Dr. David Michaels, epidemiologist and the longest-serving OSHA head from 2009 to 2017, testified at the OSHA hearing on April 28, 2022.
Beyond that, of course, we have this problem that they've really clung to this, what we call the droplet dogma that clearly has been shown to be incorrect, certainly by the research by several of the people on this panel who've done remarkable work as you heard from Dr. Prather and Dr. Milton in particular. Look, it's disappointing. I think the whole country is disappointed. But um, you know, you need employers need to know exactly what to do, or how to at least process the challenge that they face to protect workers. And OSHA standards tell employers how to do that. They say this is what we expect you to do. We expect you to develop a plan, the plan has to take your situation into account, but also has to ensure that you're looking at the hierarchy of controls, you're thinking about engineering controls first, all of those things are missing from CDC recommendations. And finally, I think I talked about this in my testimony, OSHA has a statutory responsibility, statutory requirement to have an open and transparent process like we are having today to to determine what the standard should be. CDC is a black box. We have no idea how these recommendations are determined. Unfortunately, until there are Freedom of Information Act requests or congressional inquiries. So given all those things, it's really incumbent upon OSHA to develop standards and to say these are the standards that every employer covered by the standard must follow. Thank you, Dr. Michaels.
In February 2021, there was an AP News article that with the headline, hospitals still ration medical N95 masks as stockpiles swell. And I'm going to quote, internal government emails attained by the Associated Press show that there were deliberate decisions to withhold vital information about new mask manufacturers and availability. Exclusive trade data and interviews with manufacturers, hospital procurement officials, and frontline medical workers reveal a communication breakdown, not an actual shortage. That is depriving doctors, nurses, paramedics, and other people risking exposure to COVID-19 of first-rate protection. Before the pandemic, medical providers followed manufacturer and government guidelines that called for N95s to be discarded after each use largely to protect doctors and nurses from catching infectious diseases themselves. As N95s ran short, the Centers for Disease Control and Prevention modified those guidelines to allow for extended use and reuse only if supplies are depleted, a term left undefined. Hospitals have responded in a variety of ways, the AP has found. Some are back to pre-COVID-19, one use per patient N95 protocols, but most are doling out one mask a day or fewer to each employee. Many hospital procurement officers say they are relying on CDC guidelines for depleted supplies, even if their own stockpiles are robust. The CDC knew about aerosol transmission. They had put out guidance for respirator N95s and elastomeric respirators in September of 2017. What seems to have happened is that the minute there was business pressure, all of these really good pandemic plans and pandemic measures and recommendations, that all got thrown out the minute there was any business pressure. It was basically, go back to normal. Get into the economy. Everybody get back out there. Spending. Going to restaurants. We have to all sacrifice ourselves on the altar of The Economy as a false god. And. That's what precipitated all this. It wasn't that people didn't know what to do. It wasn't that we had public health people who didn't understand what needed to be done. It wasn't that nobody understood how COVID spread. Everybody knew this. There was substantial pressure to not do those things. Just not do them. And that led to what we're seeing is that Then they have to work backwards and reverse engineer it and say, oh, we just didn't know. And it reminds me of the elite panic. We're always back to elite panic, aren't we? We always come back to elite panic. The reporter Walker Bragman and Alex Koch had done extensive research on the funding and what was going on behind the scenes there and this is a quote from their article How the Koch Network Hijacked the War on COVID from December of 2021. Quote, The decline in in-person shopping and work combined with factory shutdowns in places like China disrupted the economy. A 2020 report from the corporate consulting firm McKinsey & Company found the hardest hit industries would take years to recover. One sector in particular that took a big hit was the fossil fuel industry. Oil demand fell sharply in 2020. Placing the global economy on uncertain footing. Before long, business-aligned groups, particularly those connected to fossil fuels, begin targeting the public health measures threatening their bottom lines. Chief among them were groups tied to billionaire Charles Koch, owner of Koch Industries, the largest privately held fossil fuel company in the world. The war on public health measures began on March 20, 2020, with Americans for Prosperity, the right-wing nonprofit founded by Charles and David Koch, issued a press release calling on states to remain open. And it has been this way, and we know that a lot of the public health measure resistance, manufacturing mild, and all of that is all business oriented. It's all coming from business interests and also eugenicist kind of political ideology. Now why, you might ask, why is this mattering as far as infection control in hospitals? Like surely hospitals have nothing to do with that. Well, first of all, if hospitals have to control infection, they have to invest money in that. So the hospital industry doesn't want to do that. They don't want to pay for masks. They don't want to pay for tests. They don't want to hold up lucrative elective surgeries and procedures that get delayed or permanently put off by somebody having COVID. And so there's that. And then also, it's just that if there's masks in health care, that reminds people that the danger exists. Because if they're worried about COVID spreading in hospitals, obviously, we know that COVID is still spreading. So that's another issue. And like that Twitter rando had said, You want to remove masks everywhere so people don't live in fear. Voila! Roaring economy. Spending is about freedom. Happiness is freedom from fear. A billboard that screams whatever you're doing is okay. And we know that they're trying to get the last of the concerned people out there quote-unquote out there into the economy because there's articles written about this. In MarketWatch, there was an article in December 2022, the headline says people are, quote, long social distancing due to COVID-19. Economists say that's contributing to a drop in labor force participation. And a quote from that is, knowing that COVID-19 has not gone away, some people are not yet prepared to let down their guard. According to a working paper distributed by the National Bureau of Economic Research, some 13% of U.S. workers said they will continue social distancing as the economy opens up and cases fall, and another 45% said they will do so in limited ways. Project 2025 the presidential transition project mandate for leadership the conservative promise published in 2023 by the Heritage Foundation the think tank that informs Republican lawmakers and that says about masks in health care and it says quote refrain from opposing general COVID-19 mask mandates in healthcare facilities or personnel. So as you see, they're trying to get rid of masks in healthcare and stop based on very confused and wrong. They contradict themselves. They say that the disease is endemic and constantly mutating. However, refer to supposed natural gained immunity. Yeah, they don't make sense. And where a disease is endemic, you have permanent infection controls. We don't say, oh, malaria is endemic, let's just let the mosquitoes eat us alive. We don't do that. But the Republicans apparently want us to. So there you go. Going back to the Medpage Today article, there were some comments that I wish they had made to the HICPAC public comment. One of the comments said, quote, with guidelines like that, it just sounds as though CDC is attempting to ensure its own future existence. And this is a comment by Dr. Kaitlin Sundling.
Hello, my name is Kaitlin Sundling. I'm a physician, scientist and pathologist in Wisconsin. I have no conflicts of interest to disclose. I'm a member of the People's CDC. I'm speaking today in support of universal masking and healthcare ideally with broad use of well-fitting N95 or better respirators as a new addition to standard precautions. Now is the time to use what we've learned from HIV and blood-borne pathogens matching our understanding of the science of aerosol transmission to our precautions and healthcare allows us to work to build public trust and de-stigmatize aerosol transmitted infectious diseases, especially where asymptomatic transmission is common, as with COVID. Denying the well-proven science of N95 respirators would be a significant step backwards. There is no physical basis to support the idea that different aerosol pathogens travel different distances. Appropriate isolation for known or suspected aerosol pathogen infections of any kind, including COVID, must include N95 respirators at minimum and appropriate ventilation controls. I want to share a couple of experiences where universal airborne precautions would have prevented exposure from my own work as a pathologist and as medical director of a health professional training program. While I was in my fellowship training at a well-known Boston hospital, I found out I had been exposed to tuberculosis when I had performed a small biopsy of a neck lymph node on a patient who, as far as we knew, lacked any symptoms or history that would have caused us to suspect the infection. More recently, one of my students was also exposed to tuberculosis on a lung biopsy procedure where cancer had been the suspected diagnosis. If we only protect ourselves against known or certain exposures, we put both patients and workers at risk. We need to expand, not reduce, the use of N95 or better respiratory protection, including elastomeric respirators with source control and PAPRs in healthcare settings. Lastly, and most importantly, we have a duty to protect our patients. I've had multiple people in my community ask if I, as a pathologist and laboratory-based clinician, can be their primary care provider. It is incredibly sad to me that so few of my fellow healthcare providers are wearing masks to protect themselves and their patients, and some are not even willing to mask upon request. Where providers are masking, our patients, including those who are immunocompromised, still face unmasked waiting rooms and other spaces with shared air. Should patients have to ask their surgeon to wear sterile gloves? Putting the burden of protection on patients is not an appropriate infection control approach. In conclusion, I call on you, members of the CDC's HICPAC committee, to recommend universal masking in healthcare, ideally with the broad use of well-fitting N95 or better respirators, as a new addition to standard precautions. Thank you.
It's a shame more people were not allowed to give public comment at the meeting. But there are more people who did speak at a World Health Network YouTube video that recorded their comments and the People's CDC has been collecting written comments to share and I will end with my own public comment that I submitted in writing and I recorded on my own time
My name is Chloe Humbert I don't want to be forced into exposure to multiple infections when I need to seek health care. I almost died from infection twice in my life because of inadequate investment in health care in two different countries. If we are to be forced into preventable exposure to COVID and other diseases in health care settings against our will, the goal of this forced infection needs to be spelled out. along with clearly stating the known consequences so that the American people can say whether or not we want to bear those consequences. You can't just rip away the freedom of individuals to protect ourselves from disease and not have a clearly articulated reason because the masks off, let it rip plan sounds an awful like the natural herd immunity garbage we heard in 2020 and the American people said no to that. There are other names for this ideology and it's a pseudoscience that patriots like my father, my uncle and my stepfather all fought in a war to protect us from 80 years ago. Do not make guidelines that give cover for genocidal negligence in our hospitals and nursing homes. People in healthcare settings need to wash their hands and put on a mask and have air quality engineering controls to prevent disease spread in healthcare settings. Universal masking and broad use of N95 respirators in healthcare and essential spaces is a simple and valuable investment to save lives. And that's what I think we should do as a civilization.